Diagnosis and Staging
Initial Diagnosis – finding out you have cancer
About half of kidney tumors are found during a CT scan or X-ray. Some kidney cancers are found after certain symptoms lead to testing. Other kidney cancers are found by chance, while the doctor is looking for something else.
Testing for a Kidney Cancer Diagnosis
Doctors can do different tests to find out how much cancer is in your body. These tests can also help you and your doctor create your treatment plan. Your primary care doctor may have already done some of these tests for your initial diagnosis. However, a kidney cancer specialist may need to redo some or all of these tests.
If you have a kidney tumor, a kidney cancer specialist or team of specialists will do tests to find out:
- The size of the tumor
- If the tumor is cancerous
- If any cancer cells have spread to other parts of your body
- What treatment options are available
Tests or exams may include:

Physical exam to check your overall health
This could include checking vital signs like:
- Blood pressure
- Temperature
- Weight
- Pulse (heart beats)

Complete medical and family history
Your healthcare team will ask you about medicines you take, any other health conditions, and results of your health tests. They will want to know if any family members have had kidney cancer or other diseases.

Blood tests
Your team will take samples of your blood to check how well your kidneys are working and your overall health. Some blood tests include:
- Complete Blood Count (CBC) test – this measures the number of cells in the blood such as red blood cells, white blood cells, and platelets.
- Blood chemistry tests – these look at how well your liver and kidneys are working, and electrolytes like sodium and potassium.

Urinalysis
A test of your urine (pee) that looks for blood, extra proteins, or infection
Computed Tomography (CT) Scan
An imaging test that uses X-rays to create detailed images of certain areas of your body. It helps doctors find cancer. They will scan your abdomen (belly) and pelvis to show your kidneys and nearby areas to see if the cancer has spread.
- Before your scan, you may get contrast (a substance that you take by mouth or get injected into a vein) to improve the quality of the imaging pictures. Tell your doctor if you’ve had any reaction to contrast or iodine in the past
Magnetic Resonance Imaging (MRI)
An imaging test that uses radio waves and powerful magnets to take pictures of your body. An MRI is used to check if kidney cancer has spread to major blood vessels or the brain.
- During an MRI you will need to lie still in an enclosed space for 15 – 90 minutes. Before your doctor schedules an MRI, tell them if you’re anxious about being in an enclosed space. They may have options to make you more comfortable during the MRI.
- If you have metal in your body, such as a hip replacement or pacemaker, let your doctor know.

Bone scan
An imaging test that can show if the cancer has spread to your bones.
- Before the scan, a small amount of radioactive material is injected into a vein. It takes about 3 hours for the material to enter your blood. Doctors use a special camera to take pictures of the material in your bones.

Chest x-ray
An imaging test to see if the cancer has spread to your lungs. If something shows on the X-ray, your doctor may order a CT scan of your chest for a better look.

Biopsy
A procedure where a doctor removes a small sample of your tumor with a needle. Your team examines the sample to see if it is cancerous.
- A doctor (a urologist, surgeon, interventional radiologist, or another doctor) will insert a long thin needle through your skin into the tumor and remove a small sample.
- A pathologist at a lab will look at the tissue under a microscope to see what the cells look like and make a diagnosis.
- If the cancer has spread, your team may biopsy a sample from other areas of your body.
Based on imaging test, some patients won’t have a biopsy and will go straight to surgery. Your doctor will decide what is the best way to determine if you have kidney cancer.
Watch presentations from experts to learn more:

Types of Kidney Tumors
Benign Kidney Tumors
Benign kidney tumors are not cancerous and will not spread to other parts of the body, but they can grow and cause problems. Doctors can use many of the same treatments (such as surgery or radiation) to treat benign kidney tumors that they use for cancerous kidney tumors.
Some of the most common benign tumor types are:
- Angiomyolipoma – This is the most common type of benign kidney tumor. It often affects women or people with tuberous sclerosis, a rare inherited condition. If the tumors aren’t causing symptoms, doctors and patients may try a “watch and wait” approach. However, if they cause problems (like pain or bleeding), doctors may need to remove them with surgery.
- Oncocytoma – This is an uncommon type of benign kidney tumor. They don’t spread, but they can grow and cause other problems that require surgery. They may be related to chromophobe RCC. If you’re diagnosed with oncocytoma, your healthcare team should check you for RCC.
Kidney Cysts
A kidney cyst is a fluid-filled sac in the kidney. Not all kidney cysts are cancer.
Simple kidney cysts are small, rarely cause problems, and usually don’t need to be treated. They tend to be more common as people age. In about 40% of people (4 in 10), doctors find kidney cysts when taking CT scans or X-rays of their kidneys for other reasons.
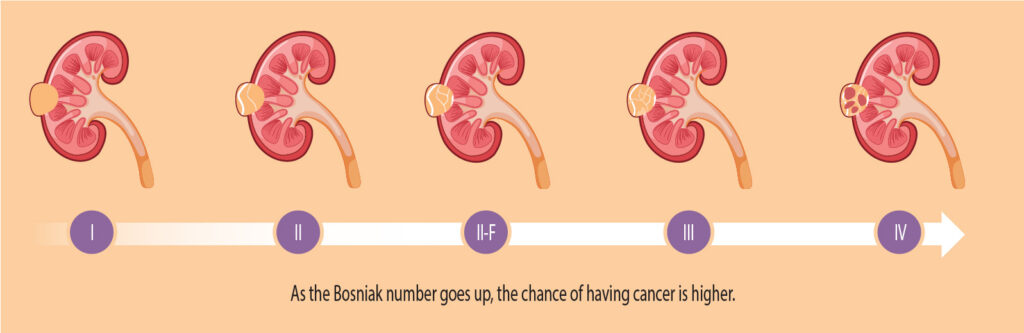
To find out if a cyst is cancer, doctors use the Bosniak classification system. This tells them if it needs to be removed, or if it can be left alone and watched. This system divides cysts into 5 categories, with Category 1 (I) as non-cancerous simple cysts that can be watched, and Category 4 (IV) as clearly cancerous cysts and should be removed. Doctors use CT and MRI scans to assign the Bosniak category.
Doctors often remove large or cancerous cysts with surgery.
Kidney Cancer
Renal cell carcinoma (RCC)
Renal cell carcinoma, also called renal cell cancer, is the most common type of kidney cancer. About 9 out of 10 kidney cancers are renal cell carcinomas.
RCC often starts as 1 tumor in a kidney, but sometimes can start as several tumors, or can be found in both kidneys at once.
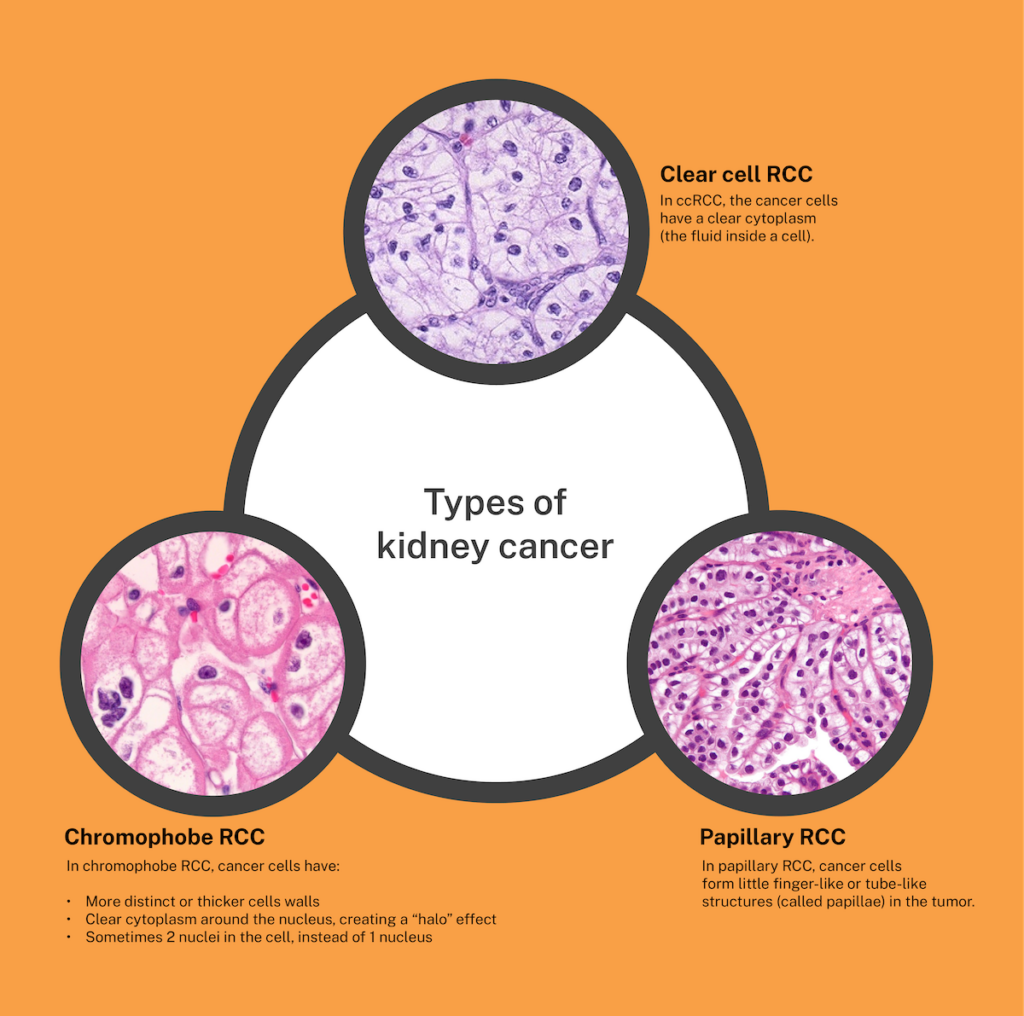
Clear cell renal cell carcinoma (ccRCC)
Clear cell RCC, or ccRCC, is the most common type of kidney cancer. About 70% of people with RCC (7 in 10) have this type of kidney cancer. It is called clear cell because the cells that make up this cancer look very pale or clear under a microscope. Clear cell RCC can be hereditary or non-hereditary.
Papillary renal cell carcinoma (pRCC)
Papillary RCC is the second most common type of kidney cancer. About 15% of RCCs (15 in 100) are this type. It is called papillary because it forms little finger-like projections (called papillae) in the tumor. Papillary RCC can be hereditary or non-hereditary.
Chromophobe renal cell carcinoma (chRCC)
Chromophobe RCC is a rare type of kidney cancer that makes up about 5% of all kidney cancers (5 in 100). It starts in the cells that line the small tubes in the kidney, which help filter waste from the blood. Chromophobe RCC can be hereditary or non-hereditary. It is less likely than other RCC types to spread to other areas of the body.
Rarer RCC subtypes
These types of RCC are very rare. Each make up less than 1% of RCC cancers (1 in 100):
- Collecting duct carcinoma – A very rare and aggressive type of RCC. When a person is first diagnosed, it is usually metastatic, meaning it has spread to other parts of the body. It is more common in younger people.
- Renal medullary carcinoma (RMC) – A rare and aggressive cancer that attacks the kidney. This cancer causes more deaths than other kidney cancers because it quickly spreads to other organs, often before it’s diagnosed. Less than 5% of patients (5 in 100) diagnosed with RMC will live beyond 3 years. This cancer is found almost always in young Black people with sickle cell trait.
- Translocation RCC – A rare type of kidney cancer that usually grows slowly. It is caused by a gene called TFE3 being broken apart and rearranged. This type is more common in children and young adults.
- Unclassified RCC: They are very rare and do not easily fit into one of the more common subtypes. They tend to be more aggressive. You may see it written on a pathology report as “NOS”, which stands for “not otherwise specified”.
Other types of kidney cancer
Wilms tumor (or nephroblastoma)
Wilms tumors are the most common type of kidney cancer in children. In children, they make up about 5% of all cancers (5 in 100) and 90% of kidney cancers (9 in 10). It most often affects children ages 3 to 4. The most common symptom is a sudden swollen stomach. Learn more from KCA’s Affiliate organization the Wilms Cancer Foundation.
Renal sarcoma
This is a rare type of kidney cancer that starts in the kidney’s blood vessels or connective tissue. There are many subtypes of sarcoma that could affect the kidney, including leiomyosarcoma, angiosarcoma, and malignant rhabdoid tumor. Learn more about sarcomas from the Sarcoma Foundation of America.
Diagnosed with transitional cell carcinoma (TCC) or upper tract urothelial carcinoma (UTUC) of the renal pelvis? While this cancer was found in a part of the kidney, it acts like and is treated similar to bladder cancer. Learn more from the Bladder Cancer Advocacy Network.
To learn more about how kidney cancer may be described by a pathologist, see a sample pathology report.
Kidney cancer that has spread to other parts of the body
In advanced kidney cancer, cancer cells can spread to other parts of the body. This is called “metastasis.” The most common sites of metastasis for kidney cancer are the liver, bones, lungs, and brain.

Kidney Cancer Stages and Grades
After you have been diagnosed with kidney cancer, doctors will try to find out the stage and grade of your cancer. This helps doctors better understand your cancer and guide your treatment.
What is a cancer stage?
A cancer stage describes how much cancer has been found in your body. For example, an early-stage cancer is only in the kidney, while a later stage cancer has spread to other areas of the body.
Knowing your cancer stage is important. It can:
- Help you understand your possible treatment options
- Help you have more informed discussions with your healthcare team
- Help you feel confident that you’re making the right decision about your health and treatment
TNM staging system
The TNM staging system is a widely used system to determine cancer stage. It stands for:
- T – Tumor: The size of your primary (main) tumor and where it is in your kidney.
- N – Nodes: The number of nearby lymph nodes that contain cancer (lymph nodes are tiny bean-shaped organs that are part of your immune system and help your body fight infection).
- Cancer in the lymph nodes is a cause for concern because when there is cancer in the lymph nodes, that cancer is more likely to spread to other organs.
- M – Metastasis: If the cancer has metastasized (spread) to other parts of your body.
When doctors stage your cancer with the TNM system, they will also add numbers after each letter that give more details about your cancer—for example, T1N0MX or T3N1M0. Here’s what the letters and numbers mean:
Primary tumor (T)
- TX: Main tumor cannot be measured.
- T0: Main tumor cannot be found.
- T1, T2, T3, T4: Refers to the size and/or extent of the main tumor. The higher the number after the T, the larger the tumor or the more it has grown into nearby tissues or major veins. T’s may be further divided to give more detail, such as T3a and T3b.
Regional lymph nodes (N)
- NX: Cancer in nearby lymph nodes cannot be measured.
- N0: There is no cancer in nearby lymph nodes.
- N1: Cancer has spread to nearby (regional) lymph nodes.
Distant metastasis (M)
- MX: Metastasis cannot be measured.
- M0: Cancer has not spread to other parts of the body.
- M1: Cancer has spread to other parts of the body.
Based on this information, doctors can give the cancer an overall stage. Kidney cancers are given a stage from 1 – 4:
Stage 1 (I)
Size: Smaller than 7cm (less than the size of a baseball)
What it means:
- The tumor is only in the kidney, is smaller than 7 cm across, and has not spread to nearby lymph nodes or other distant parts of the body.
- TNM staging would be: T1, N0, M0
Stage 2 (II)
Size: Larger than 7 cm
What it means:
- The tumor is only in the kidney, is larger than 7 cm, and has not spread to nearby lymph nodes or other distant parts of the body.
- TNM staging would be: T2, N0, M0
Stage 3 (III)
Size: Any size
Possible options include:
- The tumor has grown outside the kidney into the renal vein or even the vena cava, but not into the adrenal gland. It may or may not have spread to nearby lymph nodes, but not to other distant parts of the body.
- The tumor is only in the kidney, and the cancer has spread to nearby lymph nodes but not to other distant parts of the body.
TNM staging could be:
- T1, N1, M0
- T2, N1, M0
- T3, N0, M0
- T3, N1, M0
Stage 4 (IV)
Size: Any size
Possible options include:
- The tumor has grown outside of the kidney and may be in the adrenal gland.
- The tumor may or may not extend beyond the kidney or to nearby lymph nodes. But it has spread to other distant parts of the body.
TNM staging could be:
- T4, Any N, M0
- Any T, Any N, M1
What is a cancer grade?
The grade of a tumor describes how the tumor’s cells appear under a microscope. This can explain how quickly the tumor is likely to grow. Kidney cancers are given a grade from 1 – 4:
- Low Grade (Grades 1 and 2)
The cancer cells are more like normal cells. They grow slowly and are less likely to spread outside of the area where they started growing. - High Grade (Grades 3 and 4)
The cancer cells are less like normal cells. They grow faster and are more likely to spread to other parts of the body.
References:
Information on this page last reviewed: January, 2025
Keep Learning:
The Kidney Cancer Association provides educational literature for anyone impacted by kidney cancer.